
Different Techniques and Strategies used in Management of Stuttering: The techniques and Strategies are described based on these Approaches to Management of Fluency Disorder.
- Fluency Modification Techniques
- Fluency Shaping Techniques
- Cognitive Restructuring Techniques
- Instrumental Techniques
- Behavior Therapy Techniques
Fluency Modification Techniques
- Voluntary Stuttering – Bryngelson et al (1944)
- Stutter Fluency Technique (modified voluntary stuttering) – Van Raiper (1954)
- Bounce Technique (modified voluntary stuttering) – Johnson (1955)
- Shadowing – Cherry and Sayers (1956)
- MIDVAS – Van Raiper (1972)
- Anticipatory Struggle – Oliver Bloodstein (1982)
Voluntary Stuttering – Bryngelson et al (1944)
- Bryngelson et al (1944) found that the stutterers reported that their speech was out of control during stuttering and claimed that a sound or word ‘got struck’ and ‘would not come out’ i.e., it was involuntary and beyond control.
- He evolved the method of voluntary stuttering in 1944. He maintained that stutterers should confront their speech disruptions by consciously and willingly practicing voluntary stuttering. In this way the stutterers would reduce their fears of the unknown and be better able to control stuttering when it did occur.
- In accord with a proposed innate link between speech perception and production (e.g., motor theory), the study done by Saltuklaroglu et al (Percept psychophysics.2004 feb:66{2}) provides compelling evidence for the inhibition of stuttering events in people who stutter prior to the initiation of the intended speech act, via both the perception and the production of speech gestures.
- Stuttering was not inhibited during reading following passive audiovisual presentation of fluent speech.
- Syllabic repetitions can inhibit stuttering both when produced and when perceived, and we suggest that these elementary stuttering forms may serve as compensatory speech gestures for releasing involuntary stuttering blocks by engaging mirror neuronal systems that are predisposed for fluent gestural imitation.
Stutter Fluency Technique (modified voluntary stuttering) – Van Raiper (1954)
- Van Riper in (1954) modified voluntary stuttering. In this technique, the stutterer alters his speech patterns by repeating or prolonging the first sounds or syllables of non feared words.
- To aid easy stuttering he advocated cancellation, pull out and preparatory set.
- In cancellation, after stuttering, the client has to pause, analyze what he had done and determine how he could stutter differently on the same word. Then he could say the same word differently.
- The task is not to say the word fluently on the second trial, but to stutter volitionally with less abnormality.
- The rationale was that cancellation weakened involuntary symptom patterns and allowed learning of substitute forms of more fluent stuttering.
Bounce Technique (modified voluntary stuttering) – Johnson (1955)
- Johnson (1955) modified voluntary stuttering and called it as ‘the bounce’.
- Instead of the stutterer initiating his own stuttering as in voluntary stuttering, Johnson advocated that stutterers should use an easy bouncing repetition of the feared sound or word as a therapeutic technique for confronting avoidance behavior and moving forward in speech.
Shadowing – Cherry and Sayers (1956)
- A stuttering treatment technique in which the client, without seeing the text, repeats (shadow) everything the clinician reads from a book, client stays a few words behind the clinician. Typical effect is to reduce the frequency of stuttering.
- Cherry and Sayers (1956) popularized shadowing as a technique and reported good results with clients with stuttering. Feider and Standop (1983) applied shadowing by having the clinician begin with a list of short sentences spoken at a slow rate.
PROCEDURE:
- Assess the client and base rate the stuttering frequency .
- Select the reading material that is suitable to the client .
- Instruct the client to say everything that you read.
- Give practice by reading a few sentences at a time, stopping, and reinstructing, if necessary .
- Do not show the text to the client .
- Read normally, do not change the rate, rhythm, or phrasing
- Tape record the client’s shadowing to measure the frequency of stuttering during treatment sessions
MIDVAS – Van Raiper (1972)
Each Seprate letter of this word MIDVAS refers to the goal of a particular phase of therapy, and they follow the order of the letters of the word.
M for Motivation
I for Identification
D for Desensitization
V for Variation
A for Approximation
S for Stabilization
Motivation
- Motivation is the most important underlying factor throughout the therapy process.
- It is the drive to begin to take control of speech.
- The client becomes an active participant in the treatment process.
Identification
Identify both surface and intrinsic features of stuttering. With the assistance of the clinician, client making a list of “things I do when I stutter” to identify surface features of stuttering. These are the behaviors that can be observed in a mirror, recorded, and identified on video and audiotapes. Another list, “things I do because I stutter,” can include the less obvious, intrinsic features of the syndrome such as avoidances, anxieties, feelings of fear and helplessness, and the decisions and choices the speaker makes because of the possibility of stuttering. Thus identify the feature that occurs frequently during treatment. (Ex- writing autobiography)
- Client increases awareness of individual stuttering behaviors.
- This stage is especially challenging as feared behaviors once repressed are now open for discussion.
- Prior to changing a behavior, it is important to know as much as possible about that behavior.
Desensitization
For both overt (surface) and covert (intrinsic) features of his stuttering. This includes voluntary, intentional, or pseudostuttering. The clinician can often begin by asking the client to follow her in producing easy one or two unit repetitions and brief 1-2 sec prolongations. In severe case one can include struggle behaviors and blocking of airflow and voicing. Voluntary stuttering provides a way to break the link between the experience of stuttering and being out of control.
- Reduction of stress associated with stuttering.
- Empowers the individual to develop new strategies to cope with stuttering.
- Negative practice (stuttering on purpose)
- Direct confrontation
- Associating an old behavior with a more positive internal outcome.
Variation
Here the client is not asked to stop performing surface or secondary behavior but rather to vary them in some preplanned manner. That is the client may select the feature of producing a series of “ahs” prior to a feared word. Rather than attempting to cease production of the ‘ah” as a postponement or timing device as he anticipates a feared word, he could choose to systematically vary the rate, intensity, number, or vowel segment.
- Provides the individual alternative stuttering methods to increase speaking control.
- Example: Individual stutters using a novel behavior such as a whole word repetition in substitution for a tense prolongation.
- Increases individual’s control in a variety of settings.
Approximation

Alteration of stuttering behaviors in the direction of “normal” fluency.
Cancellation (Post event): Once stuttering occurs, the individual stops, pauses, and modifies the form of stuttering.
Pull out (Para event): Alteration of stuttering behavior as it is occurring.
Preparatory set (Pre event): Anticipation of stuttering behavior and modification before it occurs.
Stabilization
Newly learned modification skills are practiced under more stressful conditions both within and outside of the treatment setting, with the goal of having the speaker become resilient in response to stress and communicative pressure.
- Individual becomes a confident communicator.
- Individual possesses the skills to act as own clinician.
- Transition from individual therapy to group therapy.
Anticipatory Struggle – Oliver Bloodstein (1982)
- Use for Stuttering Type: anticipatory struggle, Manifestation tension & fragmentation
- Goal: reduce anxiety; modify stuttering behaviour
- Procedure: Relaxed, unhurried movement of articulators from sound to sound
Fluency Shaping Techniques
- Air Flow Therapies (Regulated breathing method) – Azrin and Nunn (1974)
- Flow and Slow Method (Modified Airflow) – Martin Schwartz (1976)
- Articulatory Level Therapy – Froeschels (1950)
- Continuous Phonation and Blending – Pindzola (1987)
Air Flow Therapies (Regulated breaking method) – Azrin and Nunn (1974)
Rationale: Stuttering is a habitual disorder of the initiation and maintenance of airflow and should be
eliminated if the stutterer emits speech behaviors that are incompatible with these airflow anomalies.
This method is based on the belief that stuttering is a habitual disorder of initiation and maintenance of
air flow and hence should be eliminated if the stutterer emits speech behavior that are incompatible with
these air flow anomalies. Stutterers are trained to control a wide range of aspects of air flow. These
aspects involve
- Smooth breathing.
- Exhalation prior to speech,
- Blending words into exhalation patterns
- Continued exhalation after the last sound of utterance
- Pausing at natural juncturing points
- Smooth inhalation during the prespeech pause and
- Formulation of general speech content
A brief treatment of one or two sessions each of two to three hours involves breath mananagement
practice. This is done initially in reading followed by spontaneous speech gradually decreasing the
frequency of pauses. Generalization is minimal and is restricted to the clinic and its environment.
Flow and Slow Method (Modified Airflow) – Martin Schwartz (1976)
Rationale: Stuttering is the result of excessive tensing of vocal folds before speech producing feedback
that triggers conditional struggle. To eliminate this malfunctioning, stutterers are made to relax the vocal
folds by maintaining passive airflow.
This method is based on the assumption that stuttering is the result of excessive tensing of the vocal folds before speech, producing feedback that triggers conditional struggle.
- To eliminate this malfunction, stutterers are made to relax the vocal folds by maintaining passive airflow.
- Initially, the stutterer has to initiate passive airflow prior to speech and to slow the first of each utterance.
These skills are to be practiced in increasingly long and complex utterances and finally in generalization tasks. For a year after intensive treatment, daily home assignments are carried out and audio taped sample are mailed to the clinic.
Articulatory Level Therapy – Froeschels (1950)
Light Consonant Contact (LCC): Froeschels (1950) described LCC. Every speaker develops habituated sets of articulator performance in terms of shaping (modulations in the vocal tract), force and deviation. Any distortion in any of these parameters would result in stuttering. Tension leads to be tensed, prolonged, interrupted articulatory movements.
Teaching LCC:
- Have the client utter a phrase
- Repeat the phrase with his / her mouth open as wide as possible. Production should be relaxed, not too loud and the speech should be melodic with least effort.
- The clinician can use different practice material (word lists, phrases and sentences)
Continuous Phonation and Blending – Pindzola (1987)
Prolongation is mostly used therapy procedure for clients with stuttering. Prolongation always involves an element of continuous phonation. Continuous phonation results in blending of words. Continuous phonation can be used along with LCC.
PROCEDURE:
- Ask the client to read the word (count the number or days of week) normally.
- Extend the phonation on the last sound of each word to the first sound of the next word.
- Move onto sentences, close end questions, paragraphs and so on.
- Finally, have the client speak for at a stretch using continuous phonation and blending at various contexts.
Cognitive Restructuring Techniques
- Analogies (Conture, 1990)
- The Garden Hose Analogy
- Blown up Balloon Analogy
- Lily pad/ Barrel Bridge Analogy
- Thumb and Opposing finger Analogy
The Garden Hose Analogy

Rationale: Analogies are used to help the child understand what the child must do to increase speech fluency. This helps the child to understand their speech system and visualize it.
Before understanding the analogy, the working of garden hose should be explained to the child:
- Permit water to flow out of the hose
- Minimize the amount of water that flows
- Nozzle stops flow
- Hose stops flow
- Completely stop the water from flowing out of the hose.
After the child is familiar with this concept similarities between the garden hose and our speech production mechanism should be taught.
Blown up Balloon Analogy
Rationale: analogies are used to help the child understand what the child must do to increase speech fluency. It is an excellent way to help the child understand tightness resulting from aerodynamic backpressure.

One excellent way to help the child understand tightness resulting from aerodynamic back pressure is by using a blown up balloon with the thumb and index finger of one hand on the balloon’s neck to stop the flow of air out of the balloon.
- Blow up the balloon and have the child feel the taut or tense sides of the balloon and explain this is a bit like the tension created by air pressure in the lungs and the vocal tract.
- Have the child gently squeeze the sides of the balloon and feel the changes in the pressure on the sides of the balloon.
- The child can hold the neck of the balloon and feel the pressure as the clinician squeezes the sides of the balloon.
Have the child figure out the best way to let the pressure out of the balloon, for eg by
- Pushing hands on the sides of the balloon
- Squeezing the thumb and index finger together and
- Slowly releasing the air through slightly separated finger thumb.
Lily pad/ Barrel Bridge Analogy
Rationale: Analogies are used to help the child understand what the child must do to increase speech fluency. This indicates that speech involves a smooth continuous movement from one sound to another.


- This analogy involves pretending as a Frog or the child’s jumping from one lily pad to the next to cross a stream.
- The therapist has to pretend that each pad is a letter of a short word like baby and that they have to hop from the bank to the first pad, then to the next pad and so on until they reach the other bank.
- Easy speech, repetition and stoppage could be demonstrated using this analogy.
The same idea can also be conveyed by the analogy of a floating bridge made of barrels tied to each other with rope.
Thumb and Opposing finger Analogy
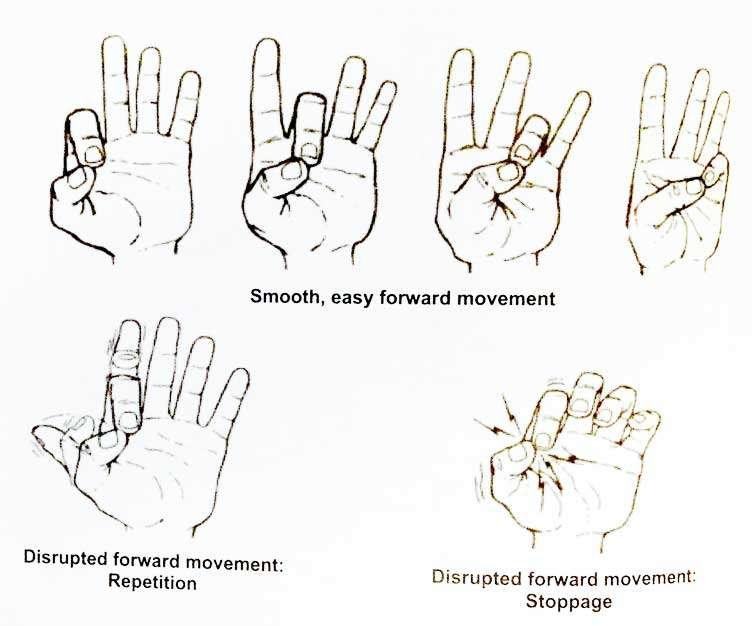
Rationale: Analogies are used to help the child understand what the child must do to increase speech fluency. This indicates that speech involves a smooth continuous movement from one sound to another.
- Each finger can be considered as a letter or sound of a short word and our opposing thumb, the tongue, or speech system, is used to produce each letter or sound.
- Fluent speech is like having the thumb move smoothly, sequentially and easy from one finger to the next.
- Conversely, stuttering is like pressing for too long with too much of force between the thumb and any one of its opposing fingers or repeatedly the thumb and one of the fingers.
Instrumental Techniques
- Delayed Auditory Feedback – Gold Diamond (1956)
- Auditory Masking – Cherry (1956)
- Metronome Timed Speech (1965)
- Unison Speech – Gregory (1968)
- Intensive Token Economy Therapy – Andrews and Ingham (1970, 1973)
- Pacing – Helm (1979)
- Dr. Fluency – Dr. Trudy Stewart and Monia Bray (1990’s)
Delayed Auditory Feedback – Gold Diamond (1956)

School-DAF
Rationale: It is based on classical behavioral approach.
- It is a method where an individual hears his own voice delayed by a few msecs through an instrument.
- It’s a good treatment for the reduction of stuttering.
- Curlee and Perkins (1969) described a therapy program in which slow, fluent speech was established by DAF of 250 msecs.
Monologue: Slow, Prolonged, Fluent Speech
Pocket DAF
Procedure:
During the early stages of therapy, DAF was set to encourage excessive prolongation, usually around 250 ms.
When clients were able to demonstrate 100 percent fluency in their speech at this delay setting, the next stepwise decrease in DAF (usually in 50 ms increments) was introduced to encourage a slightly faster rate of speech.
Again, the client learned to control fluency using decreased prolongation associated with the reduced DAF.
It is done in 7 steps.
- Reading using DAF – Start at 250 msec delay and reduce to 50 msec.
- Conversation using DAF – Start at 250 msec delay and reduce to 50 msec.
Auditory Masking – Cherry (1956)
Rationale: Listen to noise; interferes with speech monitoring; change speech behaviour
Cherry (1956) Found that masking noise can reduce stuttering with using loud masking noise. Masking noise generator unit: hearing aids – tune if/ when blocking or anticipating block.
Binaural noise masking at 95dB resulted in fluent speech. With reduced levels of noise intensity, stuttering returned.
Perkins and Curlee (1969) reported that the limitation of using auditory masking.
- Hearing loss
- Not helpful for telephone
Metronome Timed Speech (1965)
Rationale: Most AWS become more fluent, at least temporarily, when they speak using an artificial rhythm.
Procedure: Demonstrate the use of it to the client. Set the metronome at 40 beats/ min and ask the client to carry out the following:
- Tap fingers on table.
- Nod head left and right.
- Open and close jaw.
- Non sense syllables.
- Move to word level utterance each syllable to a beat.
- Sentence level: One word per beat.
Unison Speech – Gregory (1968)
- Simplest method of achieving slower rate of speech is choral speaking or unison speech, where one person (clinician) provides a vocal model to another speaker (AWS).
- Unison speech is generally used with reading aloud performance or common speaking material to both the clinician and the client.
- Pre-recorded material at various speeds can be played to the client through head phones and asked to match the rate of speech.
- The clinician overwhelm the clients own auditory feedback with his/her loud speech.
- The clinician and the client read together, moving from words to phrases to sentences and then to paragraphs.
- This recorded and played back to the client.
Intensive Token Economy Therapy – Andrews and Ingham (1970, 1973)
Rationale: A behavior punished decreases & a behavior rewarded is reinforced.
Procedure:
- In this technique initially slow rate is induced using DAF.
- Speech is then gradually shaped to normal rates in structured group conversation.
- Stutterers have to speak at specific rates at each step of therapy. No DAF is used during this stage.
- Penalty are provided for the stuttering and reward for achieving target speech rate and fluency.
- Transfer and maintenance are carried out in real life situation.
Pacing – Helm (1979)
- Some patients with SAAND may respond to pacing techniques that involve slowing the speech rate and speaking one syllable at a time.
- Often however, patients do not respond to instructions for producing slower, paced speech because of an underlying neurological drive to speak at faster rate.
- For such patients a pacing device, Helm (1979) first described had six multi colored squares with raised dividers.
- The patient was encouraged to tap his/her fore finger from square to square while speaking in a syllable to syllable manner.
Dr. Fluency – Dr. Trudy Stewart and Monia Bray (1990’s)

DR-Fluency
It is a computerized fluency shaping program.
Dr. Fluency instructs, monitors, provides feedback to the client regarding:
- Prolonged syllables
- Breathing pattern
- Gentle onset
- Reducing air pressure
- Control of volume
The management lessons in Dr. Fluency is divided into 3 parts:
Part I
- Lessons 1-4: Training in prolonged syllables
- Lesson 5: Breathing skills
- Lesson 6: Gentle onset
- Lesson 7: Reduced air pressure
- Lesson 8: Reduced Pressure on Voice Articulators
- Lesson 9: Gentle Transitions from Sound to Sound
Part II
- Lessons 10 – 11: Increasing Rate Of Speech
- Lesson 12: Continuous Speech And Volume Control
Part III
- Lessons 13: Further Increasing of Rate Of Speech
- Lessons 14: Practicing Increased Speech Rate and Normal Slow Speech
Behavior Therapy Techniques
- Fluency Reinforcement (2002, M.N Hegde)
- Response Cost for Preschoolers (2003, M.N Hegde)
Fluency Reinforcement (2002, M.N Hegde)
That stuttering may be eliminated in children by positively reinforcing fluency has been known since the
1970s (e.g., a study by Shaw & Shrum). Almost all current treatment procedures offered to preschoolers use positive reinforcement for fluency as their main component (e.g., the Lidcombe program of Onslow and colleagues).
The sequential hierarchy for treatment is as follows:
- Set the stage for fluency reinforcement
- Select effective reinforcers
- Have the parents observe the sessions
- Introduce the treatment procedure
- Begin at the sentence level
- Systematically reinforce fluency
- Use a variety of verbal praise
- Ignore stuttering
- Progression of treatment
- Reinforce fluency in continuous speech
- Reinforce fluency in narrative speech
- Reinforce fluency in conversational speech
- Use objective criteria to move from one level to the other
- Record the frequency of stuttering
- Periodically probe the stuttering rate
- Before dismissal, make sure the parents can reinforce fluency at home
- Use an objective dismissal criterion
- Follow-up the child
Response Cost for Preschoolers (2003, M.N Hegde)
Response cost is an attractive alternative to fluency shaping. It is effective with young children for whom fluency shaping is not a good option. It does not affect the speech rate and speech naturalness. It is easily administered; clinicians are readily trained in its use. Parents accept it and therefore it has high social validity.
Administration of response cost: Token award
- The clinician uses toys, story books, puzzles, selected games, activities, and so forth to evoke speech from the child.
- For every fluent production (a word, a phrase, or a sentence), the clinician places a token in the child’s container.
- The clinician also praises the child for smooth speech as she places the token in the child’s cup (e.g., Says, “That was smooth speech! Here is a token for you”)
Administration of response cost: Token withdrawal
- When the child stutters, the clinician says something like “Oh no! That was bumpy! I am taking a token back!” and removes a token from the child’s cup and places the removed token in his/ her own cup.
- The clinician fluently models the child’s stuttered production for the child to imitate and awards a token to the child if the imitated production is fluent.
Strategies used in this techniques:
Variation and progression: Initially, withdraw a token with announcement (“That was bumpy, I am taking a token back”). Later, take a token back without announcement.
Progression across response complexity: Continuous speech, narrative speech, conversational speech
Trouble shooting: Occasionally a child may react emotionally to the first token withdrawal and refuse cooperation. The child may stop talking, fight tears, leave the seat, or ask for Mommy. Serious emotional reactions need to be handled promptly and sensitively.
Reverse the Roles: The clinician plays the child’s role, and asks the child to give and take tokens for smooth and bumpy speech (and produces many bumps). Children gleefully withdraw tokens from the clinician!
Token bankruptcy: Another potential problem to be handled is token bankruptcy—the child who is left with no tokens, which means no gift at the end of the session. That, of course, can’t happen; the clinician should avoid token bankruptcy at all cost.
Handling token bankruptcy: Clinicians monitor the number of tokens the child has at any moment. When the child’s token collection is precariously low, the clinician can award two tokens for fluent and longer productions.
Parent training: Parents must be trained in the administration of response cost at home. Parent training must not be monitored in any systematic manner.
References:
⇒ STUTTERING An Integrated Approach to Its Nature and Treatment – BARRY GUITAR, PH.D. (Book)
⇒ A Handbook on Stuttering – Bloodstein (book)
⇒ Treatment Protocols for Stuttering – M. N. Hegde (Book)
⇒ Stuttering and Cluttering – David Ward (Book)
⇒ Speech Correction An Introduction to Speech Pathology and Audiology – Charles Van Riper, Robert L. Erikckson (Book)
You are reading about:
Different Techniques and Strategies used in Management of Stuttering





0 Comments