
Flaccid Dysarthrias Causes and Characteristics: Flaccid Dysarthrias are a perceptually distinct group of Motor Speech Disorders (MSDs) caused by injury or disease of one or more cranial or spinal nerves. They reflect problem in the nuclei, axons or neuromuscular junctions that make up the motor units of the final common pathway (FCP), and the manifest in any or all of the respiratory, phonatory, resonatory, and articulatory components of speech.
Causes of Flaccid Dysarthrias
Flaccid dysarthrias can be caused by any process that damages the motor unit. These include:
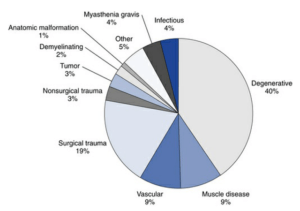
- Degenerative disease
- Trauma
- Muscle disease
- Vascular disorders
- Tumor
- Neuromuscular junction disease
- Infectious processes
- Demyelinating disease
- Anatomic anomalies and some other causes.
Degenerative Disease
Motor neuron diseases are a group of disorders that involve degeneration of motor neurons.
- Amyotrophic lateral sclerosis (ALS): It is most common motor neuron disease, affects the bulbar, limb, and respiratory muscles. ALS is a disease of both UMNs and LMNs.
- Progressive bulbar palsy: Primarily affects LMNs supplied by cranial nerves.
- Spinal muscle atrophies (sometime called Progressive muscle atrophies): It is associated with progressive limb wasting and weakness, with or without cranial nerve weakness.
- Kennedy’s disease or bulbospinal neuronopathy: It is an uncommon X-linked recessive disease that can be mistaken for ALS. It affects only males, usually after age 30, and is characterized by gynecomastia (excessive breast size), muscle cramps and twitches, limb-girdle muscle weakness, and bulbar involvement.
- Some neurodegenerative diseases with unknown pathogenesis can be associated with flaccid dysarthrias. For example, a recently described syndrome, labeled facial onset sensory and motor neuronopathy (FOSMN), appears to represent a slowly progressive neurodegenerative condition that is characterized by paresthesias and numbness in the trigeminal nerve distribution, followed by dysarthria, dysphagia, fasciculations, and atrophy indicative of lower motor neuron weakness.
Trauma
- Surgery in the brainstem or head, neck, or upper chest can temporarily injure or permanently damage speech cranial nerves and is perhaps the most common cause of vocal fold paralysis.
- Examples of neurosurgical procedures with known risks for cranial nerve damage include carotid endarterectomy, anterior cervical spine surgery, brainstem vascular procedures, and surgical resection or related procedures for tumors in the posterior fossa, skull base, or cranial nerves.
- Cardiac, chest, otorhinolaryngologic, or dental procedures directed at the heart, lungs, thyroid gland, neck, jaw, and mouth also carry risks for cranial nerve injuries.
- Closed head injury, skull fractures, and neck injuries can also cause flaccid dysarthria through trauma to cranial or cervical nerves.
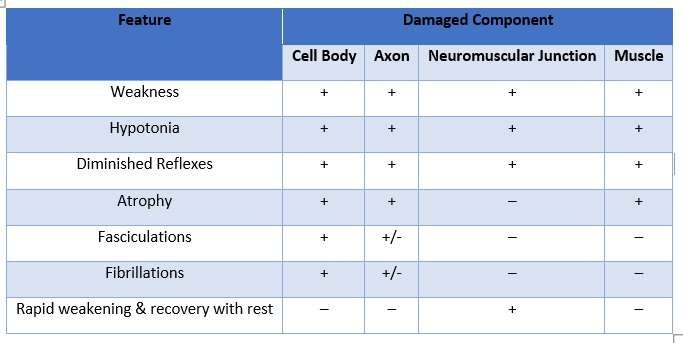
Clinical Characteristics of Flaccid Dysarthrias
Flaccid dysarthrias reflects FCP damage, reflexive, automatic and voluntary movements are all affected. Weakness, hypotonia, and diminished reflexes are the primary clinical characteristics of flaccid dysarthrias.
There are some common clinical characteristics of Flaccid Dysarthrias:
Weakness
- Weakness in flaccid dysarthria is damage to any portion of the motor unit including cranial and spinal nerve cell bodies, axon, neuromuscular junction and muscle.
- The effect of weakness on muscle can be observed during single (phasic) contractions, during repetitive contractions, and during sustained (tonic) contractions.
Hypotonia and Reduced Reflexes
- Hypotonia is reduced muscle tone, characterized by floppiness of muscle and reduced resistance to passive movement.
- Flaccid dysarthria also associated with absent or normal reflexes.
- In flaccid dysarthria, the ability of a muscle to contract in response to stretch is compromised because the motor component of the stretch reflex operates through the FCP. This results in the flabbiness that can be seen or felt in muscles with reduced tone.
Atrophy
- When cranial or spinal nerve cell bodies, peripheral nerves, or muscle fibers are involved, muscles eventually atrophy, or lose bulk.
- Atrophy is almost always associated with significant weakness.
Fasciculations and Fibrillations
- When motor neuron cell bodies are damaged and , less prominently, when their axons are damaged, fasciculation and fibrillations may develop.
- Fasciculations are visible, arrhythmic, isolated twitches in resting muscle that result from spontaneous motor unit discharges in response to nerve degeneration or irritation.
- Fibrillations are invisible, spontaneous, independent contractions of individual muscle fibers that reflect slow repetitive action potentials. They can be detected by electromyography (EMG).
- Fasciculations and fibrillations are generally not present in muscle disease.
Progressive Weakness with Use
- When disease affects the neuromuscular junction, rapid weakening of muscle with use and recovery with rest can occur.
- Common in people with any type of weakness, rapid weakening and recovery with rest are prominent in neuromuscular junction disease, such as Myasthenia Gravis (MG).
- Myasthenia gravis is an autoimmune disease characterized by rapid weakening of voluntary muscles with use and improvement with rest.
Clinical Characteristics of Flaccid Dysartrias are summarized in Table below:
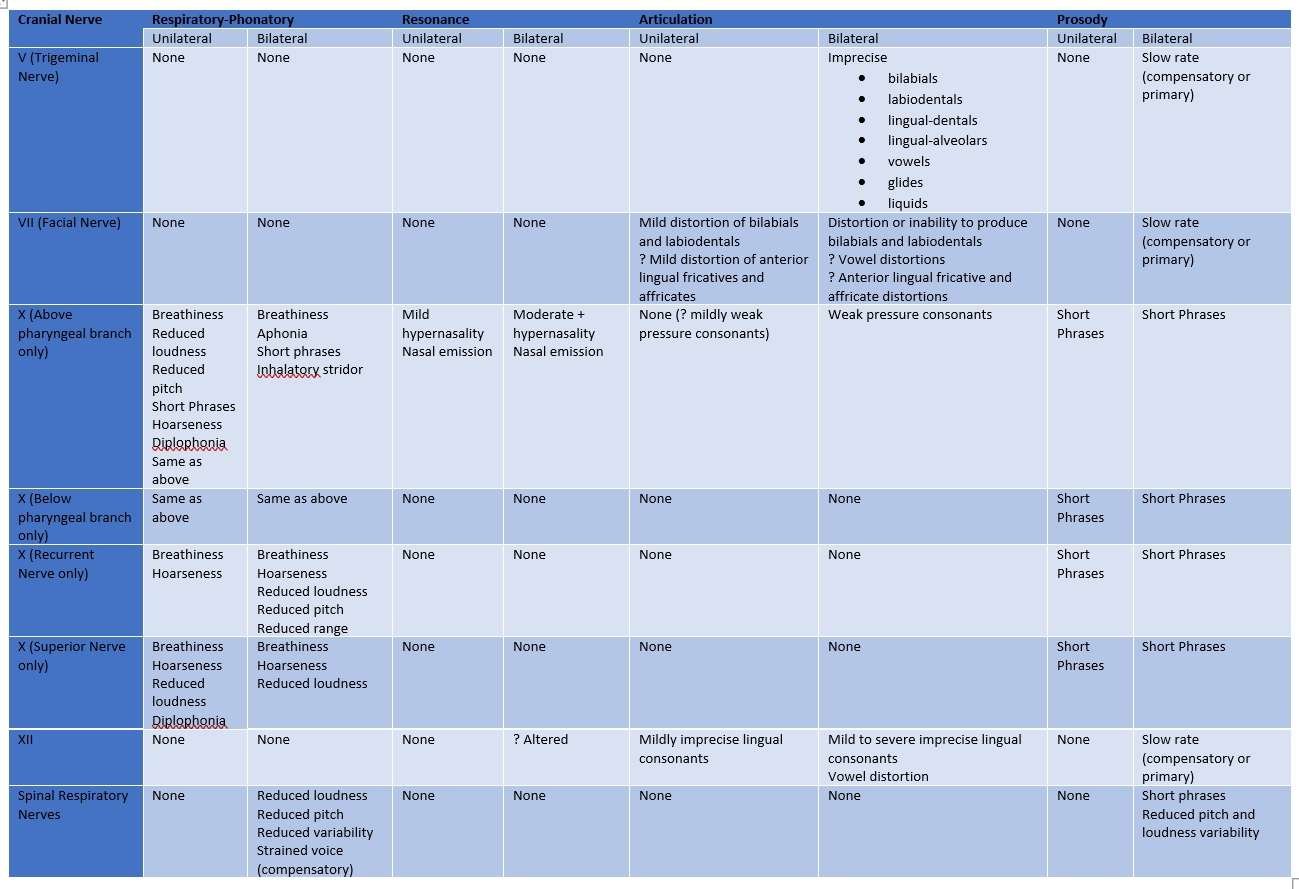
Speech Characteristics of Flaccid Dysarthrias
RESPIRATORY
- Reduced vital capacity
- Termination of speech at larger than normal lung volumes
- Larger than normal inspiratory and rib cage volumes
- Abnormal chest wall movements
- Neck and glossopharyngeal breathing
PHONATION
- Unilateral vocal fold paralysis is relatively unusual in disease processes affecting the brainstem nuclei. If unilateral damage is present, the quality of phonation depends on the position of the vocal fold.
- If it is paralyzed in an adducted position, the voice is harsh, and loudness is reduced.
- If it is in the abducted position, more breathiness is heard with reduced loudness.
- More likely is bilateral vocal cord involvement.
- The characteristics of this are a breathy voice, inspiratory stridor (or audible inhalation), and abnormally short phrases.
- Monotony of pitch and loudness is distinctive in many patients as well.
RESONANCE
- Hypernasality is noted as an outstanding characteristic of the patients with flaccid dysarthria whose disease or injury affected velopharyngeal function.
- Nasal emission of air is also found in a high percentage of those patients.
ARTICULATION
- Imprecise consonant production may be present to a mild to severe (unintelligible speech) degree.
- The consonants requiring firm contact from tongue tip elevation are particularly vulnerable.
- Plosives such as /p/, /t/, and /k/ and fricatives such as /f/ and /s/ are frequently distorted because of the lack of intraoral pressure that results from palatal dysfunction.
SWALLOWING
- Swallowing difficulty is commonly present in flaccid dysartria. The degree of swallowing difficulty and phase of swallowing (oral preparatory, oral transitory, pharyngeal, esophageal) difficulty depends on the nerve affected.
- Frequent aspiration
Speech Characteristics of Flaccid Dysarthrias are summarized in below Table:
References:
⇒ Motor Speech Disorders: Substrates, Differential Diagnosis and Management – Joseph R. Duffy (Book)
⇒ Motor Speech Disorders: Diagnosis and Treatment – Donald B. Freed (Book)
You are reading about:
Flaccid Dysarthrias: Causes and Characteristics





0 Comments